Ectopic Pregnancy: Understanding a Hard Moment, Without Fear or Blame
To anyone who has just heard the words “ectopic pregnancy,” or who fears one may be coming, the feelings that follow, fear, confusion, grief, are completely understandable. This is one of the more frightening things a person can be told in early pregnancy. What follows is a calm, honest walk through what the diagnosis means, including the parts that are hard. Two things are worth holding from the very start: caught in time, an ectopic pregnancy is very treatable, and however it came about, it is not a failing on anyone's part.
The quick answer
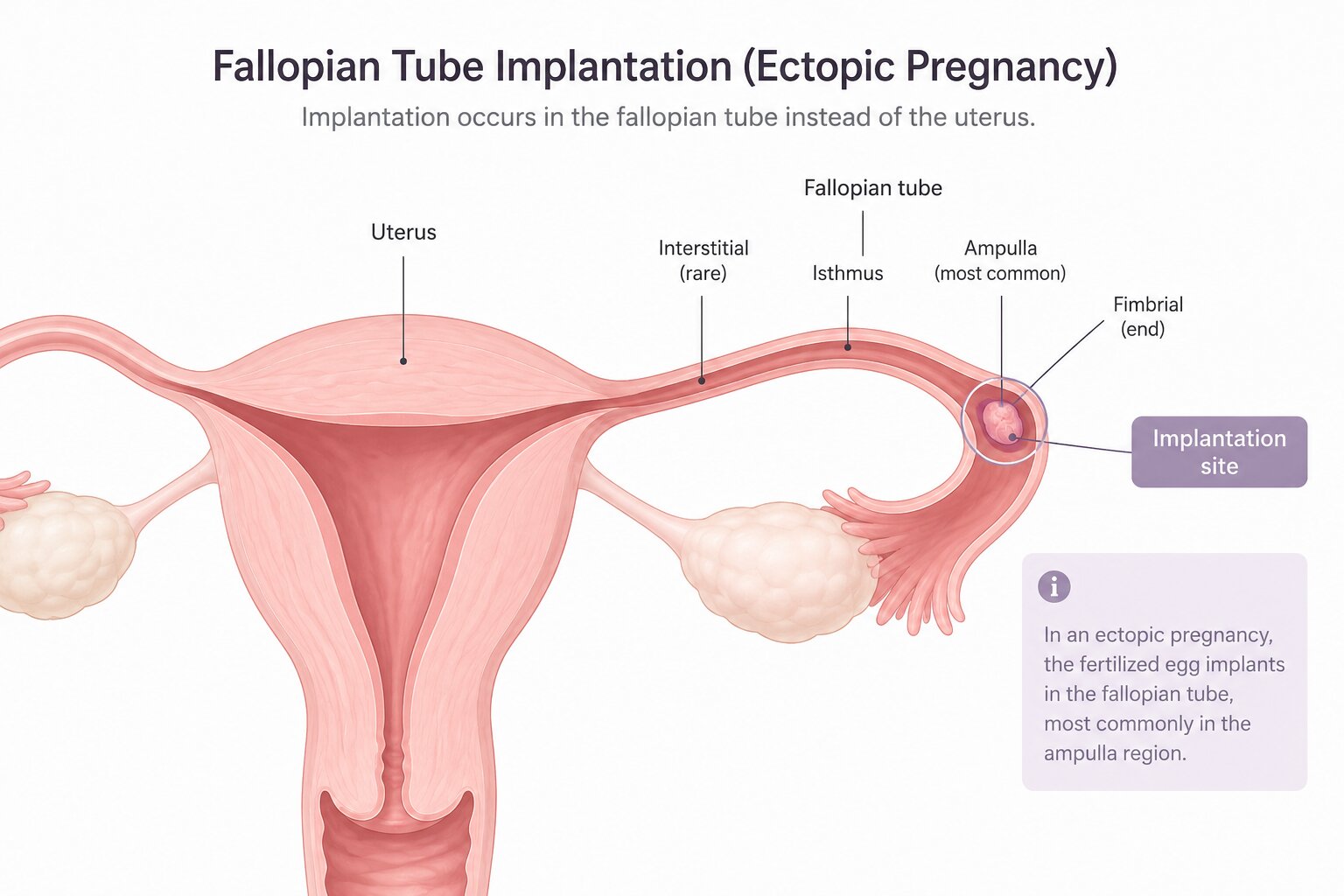
An ectopic pregnancy is one that has implanted outside the uterus, almost always in a fallopian tube. That space cannot hold a pregnancy, so it cannot continue and cannot be moved to the womb. Left unnoticed, it can rupture the tube and bleed, which is the dangerous part. But caught early, and it usually is, it is treated safely, with medicine or keyhole surgery. Most women who go through one go on to conceive again.
What matters most
- It implants outside the womb, usually in a fallopian tube, and cannot be saved.
- Caught early, it is very treatable, with medicine or minimally invasive surgery.
- The real danger is rupture and internal bleeding, which is what the emergency signs point to.
- About half of the women who have one had no risk factor at all.
- Most go on to have a healthy pregnancy afterwards, even with one fallopian tube.
- The grief that comes with it is real, and it does not need to be justified to anyone.
What an ectopic pregnancy really is
A pregnancy normally makes its way to the uterus, an organ built to expand and nurture a baby for nine months. An ectopic pregnancy never reaches that destination. Instead it takes root somewhere it was never meant to be, in around 95 out of 100 cases inside the fallopian tube itself, and occasionally on an ovary, on the cervix, or within the scar of an earlier caesarean.
This is the part that is hard to hear. A tube cannot hold a pregnancy, and there is no way to move it into the womb, so it cannot be saved. As it grows it can rupture the tube and bleed inside, which is what makes it urgent. Treatment is never about continuing the pregnancy; it is about protecting the mother. And that is a real loss, the kind one is allowed to grieve without having to explain it to anyone.
Why it happens, and why it is no one's fault
When the mind keeps circling back to what one might have eaten, lifted, or done differently, that is not weakness. It is grief looking for a reason. So here is the reason, as far as there is one: about half of all women who have an ectopic pregnancy have no risk factor at all. It happens to healthy women who did nothing wrong.
Where risk factors do exist, they usually trace back to something that quietly affected the fallopian tubes:
- a previous ectopic pregnancy,
- a past pelvic infection, such as an untreated sexually transmitted infection, which can scar the tubes,
- earlier surgery on the tubes or pelvis, or endometriosis,
- a pregnancy conceived through IVF, or with an IUD in place,
- smoking, or being over 35.
Few of those are anything a person chooses. An ectopic pregnancy is about where the pregnancy landed, not a failure of effort, care, or love.
The signs to know
Early on, it can feel like any other pregnancy: a missed period, a positive test, tender breasts, a little nausea. The warning signs usually turn up between about week 4 and week 12, often around weeks 6 to 8.
The common early ones:
- pain low in the tummy or pelvis, often on one side,
- vaginal bleeding, sometimes darker or more watery than a period.
On their own these can have gentler causes, but in early pregnancy they are worth a prompt call to a doctor. The emergency signs, which can mean the tube has ruptured, are the ones to memorise: sudden or severe pain, pain at the very tip of the shoulder, faintness or collapse, and heavy bleeding. That shoulder-tip pain is an odd but telling clue, from internal bleeding irritating a nerve under the diaphragm.
How it is found
It is usually found with two things together: a transvaginal ultrasound of the uterus and tubes, and blood tests measuring the pregnancy hormone hCG, often repeated over a couple of days to see which way it is trending. Sometimes, very early, a scan cannot yet tell where the pregnancy is, a “pregnancy of unknown location.” It sounds more ominous than it is: not a sign anything is wrong, only that a little more monitoring is needed, which is exactly what keeps a woman safe.
How it is treated
The path depends on how early it is caught, the hormone level, whether the tube has ruptured, and how the woman is. A doctor guides the choice:
- Watchful monitoring: for small, early, resolving ectopics, blood tests track the hormone falling on its own.
- Medicine (methotrexate): an injection that stops the tissue growing so the body reabsorbs it over a few weeks, no surgery. It suits unruptured cases with lower hormone levels, with follow-up tests. Any new pain, shoulder pain, or dizziness during it should be reported at once.
- Keyhole surgery: the surgeon removes the affected tube (salpingectomy), or opens and preserves it (salpingostomy). A ruptured tube means emergency, life-saving surgery.
None of these is a failure, and none is a punishment. Each is just the safest way, in a particular situation, to protect a woman's health and her future.
Trying again, later
There is one fear that sits under all the others, whether or not it is said aloud: whether this ends the chance of a baby. For the great majority, it does not. Even when a tube has been removed, the other usually takes over, and conceiving stays very possible. The chance of another ectopic is a little higher than average, which is why the next pregnancy tends to get an early scan around six or seven weeks, to confirm it has settled in the right place. When the time feels right, in body and in heart, a doctor can help think it through.
The grief that deserves space
An ectopic pregnancy is a strange kind of loss, because it comes tangled up with a medical emergency. In the rush of scans and decisions, it is easy for one's own grief to be the last thing anyone tends to, oneself included. It should not be.

It is the loss of a pregnancy. It may also have meant real fear for one's own life, or surgery, or the news that a part of the body has changed. All of that is worth grieving, at whatever pace it comes. There is no correct timeline here, and no version of this where anyone was “supposed” to feel less. Leaning on a partner, a friend, or a counsellor is not weakness; it is care. And if the sadness sits heavy or stays a long while, a doctor or a mental health professional can help find support meant exactly for this.
When it can't wait
In early pregnancy, one-sided pain or unusual bleeding is worth a prompt call to a doctor. The emergency signs above, sudden severe pain, shoulder-tip pain, faintness, or heavy bleeding, mean hospital straight away; they can signal a rupture, and quick help saves lives.
Looking ahead
In the thick of it, the horizon can be hard to see. But most women move through an ectopic pregnancy, heal in body, slowly heal in heart, and, when they feel ready, go on to have the family they hoped for. It is far more common than most people realise, and it is not a door closing. It is a hard chapter, held carefully by people whose whole job is to keep mothers safe, and followed, for most, by gentler ones.
Common questions
Can an ectopic pregnancy ever be moved to the womb?
No. There is no way to relocate it, and it cannot continue. Treatment is about protecting the mother's health.
Could anything have prevented it?
In most cases, no. About half of women who have one have no risk factor at all, and it is not caused by anything they did.
Is pregnancy still possible afterwards?
Most likely, yes, even with one fallopian tube, though the next pregnancy is watched a little more closely early on.
ParentVeda offers gentle, evidence-informed guidance, not medical advice. In early pregnancy, sudden or one-sided pain, shoulder-tip pain, faintness or heavy bleeding needs urgent medical care. Always consult your doctor for decisions about your pregnancy.
Source: Reviewed against ACOG, Mayo Clinic, RCOG / The Ectopic Pregnancy Trust and NHS patient guidance.